
Rotator Cuff Disorders - The Bigger Picture
Spinal mobility has an important role to play in shoulder function
Treating the Rotator Cuff (4 CEUs)
In 70% of all doctor and therapist visits for shoulder problems, the diagnosis is rotator cuff disorder (Lewis 2014)
The etiology of rotator cuff disease is likely multifactorial, including age-related degeneration and micro-trauma.
The incidence of rotator cuff tears increases with aging, with well over half of individuals in their 80’s having a rotator cuff tear.
Smoking, hypercholesterolemia, and genetics have all been shown to influence the development of rotator cuff tearing.
Substantial full-thickness rotator cuff tears, in general, progress and enlarge with time.
Pain, or worsening pain, usually signals tear progression in both asymptomatic and symptomatic tears and should warrant further investigation. Larger (>1-1.5 cm) symptomatic full-thickness cuff tears have a high rate of tear progression and, therefore, should be considered for earlier surgical repair in younger patients only.
If the tear is repairable and there is limited muscle degeneration, surgery should help to avoid long-standing irreversible changes of the cuff.
Smaller symptomatic full-thickness tears have been shown to have a slower rate of progression (similar to partial-thickness tears), and are more suited to hands-on treatment and exercise due to the limited risk for rapid tear progression.
In both small full-thickness tears and partial-thickness tears, increasing pain should alert you to obtain further imaging, as it can signal tear progression.
Surgery
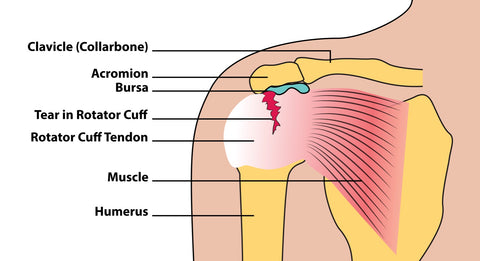
Traditionally, many orthopaedic texts talk of tendon tears typically occurring due to rubbing of the tendon on the acromion or a spur. This has given rise to operations such as decompression or acromioplasty, where a piece of the acromion is removed.
Interestingly and IMPORTANTLY however, the evidence says otherwise. Ultimate failure stress of the bursal side is double that of articular side fibers. This may mean that many shoulder operations (estimated $3bn per year, USA) may be totally unnecessary and are not supported by the evidence!
Remember the Thoracic Spine
Spinal mobility has an important role to play in shoulder function, especially the thoracic spine. Improving thoracic spine mobility can have a hugely beneficial effect on rotator cuff function. A stiff or kyphotic (rounded) thoracic spine should be addressed with soft tissue work, self-help exercise and mobilization techniques.
Posture & Lifestyle
There are specific activities and maladaptive postures that serve as trigger point activators, either promoting ‘new’ trigger points to develop or causing latent ones to become active. These may cause a previously asymptomatic shoulder muscles to develop pain.
For example:
• Standing or sitting in a slouched position
• Sitting with legs crossed
• Leaning the head to one side in a telephone position is a problematic posture
• Any job where there’s a lot of lifting and carrying
• Working above the head for an extended period of time (including swimmers, tennis players, painters, flight attendants, mechanics, and decorators).
In support of the above, Svendson (2004) published an MRI study, which concluded that people who work with their arms above their heads have a 100% chance of developing degeneration of the rotator cuff tendons.
Janda (1996) identified ‘the upper crossed pattern’ with tight and short anterior chest muscles and weak overstretched posterior shoulder muscles.
Tsai et al (1998) showed that altered thoracic and cervical curvature (either structural or functional) causes early muscle fatigue. Head forward posture and scapular protraction have both been associated with sub-acromial impingement.
More recently a March 2015 study examined 379 residents in a Japanese Village during annual health checks using ultrasound examination. The conclusions where definitive:
“Postural abnormality represented an independent predictor of both symptomatic and asymptomatic rotator cuff tears. These results may help define preventative measures for rotator cuff tears and in the design of rehabilitation therapies for shoulder disease.”
We can therefore see that treating shoulder pain needs to be holistic and that shoulder function will compensate for problems elsewhere in the body.
Causes in Context
Performing mechanically efficient shoulder activities requires the rest of the body to function optimally. Kibler (1995) analyzed the biomechanics of the tennis serve and demonstrated that 54% of the power comes from the legs and trunk. Here is the breakdown:
• Leg/Trunk 54%
• Shoulder 21%
• Elbow 15%
• Wrist 10%
This example of the shoulder in action (tennis serve) clearly demonstrates how a problem with a leg, trunk, elbow or wrist - or even arthritis of the big toe - will need to be compensated for during shoulder intensive activities.
Conclusion
As bodyworkers we are encouraged to view our patient’s symptoms in context. The presenting symptom is sometimes the tip of an iceberg.
Patients often manifest a soft tissue protective ‘holding pattern’ around the problem area. This holding pattern is a result of the ‘switching off’ of functional units to avoid noxious stimuli (such as pain).
We palpate this switching off as muscular conflict. Add to this, postural or habitual issues and we will gain a clearer picture of our patients’ issues in context.
Trigger points, insofar as we accept them as part of the body's natural protect and defense mechanism, are often a good indicator of postural issues.
Early identification and treatment is therefore always likely to be beneficial.
Find a Trigger Point Professional in your area
Dry Needling for Trigger Points
Certify as a Trigger Point Therapist
Nationally Accredited Home Study Courses:

This trigger point therapy blog is intended to be used for information purposes only and is not intended to be used for medical diagnosis or treatment or to substitute for a medical diagnosis and/or treatment rendered or prescribed by a physician or competent healthcare professional. This information is designed as educational material, but should not be taken as a recommendation for treatment of any particular person or patient. Always consult your physician if you think you need treatment or if you feel unwell.
