
Trigger Point Therapy - Fibularis/Peroneus

Trigger points in the Fibularis/Peroneus muscles of the lower leg are a common, but often over-looked, source of ankle pain and weakness
Anyone who suffers from frequent and reoccurring ankle sprains is likely to have trigger points in these muscles.
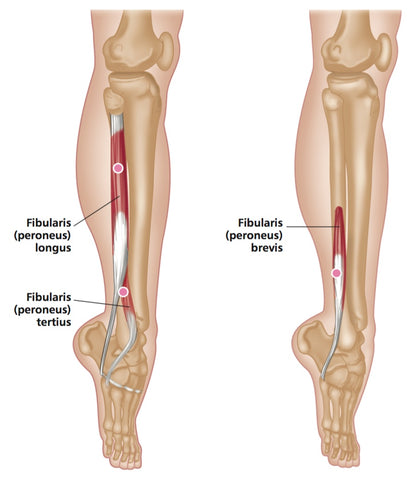
FIBULARIS - ANATOMY
The course of the tendon of the insertion of the fibularis longus helps maintain the transverse and lateral longitudinal arches of the foot.
A slip of muscle from the fibularis brevis often joins the long extensor tendon of the little toe, whereupon it is known as peroneus digiti minimi.
The fibularis tertius is a partially separated lower lateral part of the extensor digitorum longus.
ORIGIN
Longus: upper two-thirds of lateral surface of fibula. Lateral condyle of tibia.
Brevis: lower two-thirds of lateral surface of fibula. Adjacent intermuscular septa.
Tertius: lower third of anterior surface of fibula and interosseous membrane.
INSERTION
Longus: lateral side of medial cuneiform. Base of 1st metatarsal. Brevis: lateral side of base of 5th metatarsal.
Tertius: dorsal surface of base of 5th metatarsal.
ACTION
Longus: everts foot. Assists plantar flexion of ankle joint. Antagonist: tibialis anterior.
Brevis: everts ankle joint.
Tertius: dorsi flexes ankle joint. Everts foot.
NERVE
Fibular (peroneal) nerve, L4, 5, S1.
BASIC FUNCTIONAL MOVEMENT
Examples: walking and running; walking on uneven surfaces.
TRIGGER POINT REFERRED PAIN PATTERNS
Mainly over lateral malleolus, anteriorly and posteriorly in a linear distribution. Laterally along foot, occasionally vague pain in middle third of lateral aspect of lower leg.

Fibularis - Trigger Point Referred Pain Pattern

Fibularis - Trigger Point Referred Pain Pattern
INDICATIONS
Pronation of feet, repetitive inversion/eversion injury, tenderness around malleolus, ankle weakness, post-fracture (and casting) rehabilitation, foot problems (e.g. calluses, verrucae, neuromas), osteoarthritis of toes, metatarsalgia, ankle stiffness, lateral compartment syndrome.
CAUSES
Direct trauma, post-fracture, twisted ankle, ill-FItting boots/shoes, poor orthotics, walking on uneven surfaces, splinting (cast), sports (e.g. running, soccer, cycling, climbing, swimming), footwear (high heels), tight socks, prolonged crossed legs, sleeping on stomach with pointed toes.
DIFFERENTIAL DIAGNOSIS
Rupture. Fracture of foot. Fracture of 1st metatarsal (styloid process). Foot problems. Fibular head dysfunction (common peroneal nerve). Toe problems. Ankle problems (arthritis). Gait dysfunction. Compartment syn- dromes (lateral). Osteoarthritis of hip.
CONNECTIONS
TFL, gluteus minimus, extensor digitorum longus/brevis, extensor hallucis brevis.
COMMONLY APPLIED TREATMENT TECHNIQUES
| Deep Stroking Massage | Yes |
| Compression | Yes |
| Muscle Energy | Yes |
| Positional Release | Yes |
| Spray and Stretch | Yes |
| Dry Needling | Yes |
| Wet Needling | Yes |
SELF HELP
Self-massage techniques can be helpful. Balls and pressure tools may be used, as the muscles are superficial.
GENERAL ADVICE TO CLIENTS
Avoid high-heeled/ at shoes. Regular stretching with hot and/or cold. Strapping/ankle support. Use of heel wedges and/or orthotics. Posture and gait advice. Examine shoes.
Find a Trigger Point Professional in your area
More Articles About Ankle Pain
Certify as a Trigger Point Therapist
Education Membership Plans from $19.95/monthly

NAT TRIGGER POINT THERAPY DIPLOMA COURSE

EDUCATION MEMBERSHIP PLANS
UNLIMITED ACCESS
FROM $19.95/monthly
