
Trigger Point Therapy - Treating Spondylolisthesis
Trigger Point Therapy Treatment for Spondylolisthesis
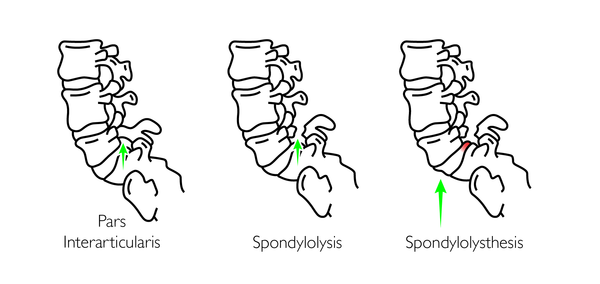
Spondylolisthesis is a fracture and slippage of a spinal vertebra (usually lower lumbar). It can develop for a range of reasons and can vary in severity.
The majority fall into one of two categories - Traumatic or Degenerative.
Whatever the underlying reason, the result is that the vertebrae literally slip either forward on the one below (Anterolysthesis) or backwards (Retrolysthesis).
This can sometimes be felt as a palpable ‘step’ as you run your fingers down the patient's spine.
Degenerative Spondylolisthesis
Usually due to aging, a degenerative spondylolisthesis happens where the spine’s support system (bones, joints and ligaments) weaken and are no longer able to maintain alignment.
Degenerative spondylolisthesis is most common in the 5th decade onwards and usually occurs at the L4/5 zone because that’s mechanically weaker due to the maximal angle of the lumbar lordosis.
This is sometimes also called a ‘stress fracture’; with the incidence increasing over the age of 40, and 5 times more common on women than men.
Traumatic Spondylolisthesis
Traumatic spondylolisthesis usually affects the lower part of the spine, most commonly the 5th lumbar vertebra (82%), but sometimes the 4th lumbar vertebra.
The usual mechanism is that a child or youth falls heavily onto the coccyx region and the cartilaginous pars splits. This type of fracture usually occurs around 5‐7 years of age, however the symptoms may not often be felt until adulthood.
Usually a traumatic slippage is a grade I or II and is well adapted and compensated for by the body over time.
However, it is not uncommon to see young boys (mainly) of 14/15 years old coming to you with acute spondylolisthesis‐induced low back pain.
Common Symptoms
Patients typically have complaints of pain in the back with intermittent pain to the legs. Spondylolisthesis can often cause muscle spasms, or tightness in the hamstrings.
Symptoms will depend on a number of factors, age, chronicity and the degree/grade of slippage.
We grade slippage from I‐IV according to the percentage of slippage, and as the bone slips it can also pull on the intervetbral disc, which can be a source of pain.
Remember that most spondylolisthesis’ occur at the L5/S1 level.
Anatomically most of the spinal nerves have exited to the lower extremities by the L3/4 zone (the cauda equina starts at L2/3), so any nerve damage or symptoms will tend to be less serious than if the slippage was higher up.
Can be mistaken for Sciatica or Pseudo-sciatica
Spondylolisthesis can affect one side (unilateral) or both sides (bilateral) and often presenting as sciatica or pseudosciatica.
If severe it can also cause Cauda Equine Syndrome (CES). CES is potentially very serious and may present as a loss of bladder or bowel control/regulation, in which case you must urge the patient to seek immediate medical intervention.
Common Symptoms (may include):
• Difficulty standing straight
• Back or buttock pain
• Pain that runs from the lower back down one or both legs (sciatica)
• Numbness or weakness in one or both legs
• Difficulty walking
• Leg, back, or buttock pain that gets worse on bending over or twisting
• Loss of bladder or bowel control, in rare cases
• Pain getting up from a chair
• Morning pain and stiffness
• Back pain getting worse as the day goes on
• Pain usually is provoked by activity, particularly back extension activities
• Poor tolerance of activities requiring excessive spine loading, including running and jumping
• Sitting usually is better tolerated
• A large percentage of patients with spondylolysis are asymptomatic.
So what are the symptoms telling us?
Pain is a signal that something is wrong – it’s part of our ‘protect and defend mechanism’.
In spondylolisthesis, back pain is the most common symptom; this is mainly due to overloaded lumbar erector spinae and or multifidus muscles.
The muscles are being asked to do two jobs at the same time —the normal job of maintaining posture (multifidus) and extending the flexed spine (erector spinae) PLUS the job of stabilizing around the fracture site.
This causes muscle fatigue and low grade constant aching, which is also one of the reasons why the lower back pain is often worse during the day.
Muscle Fatigue
As the muscles fatigue, the pressure on the spinal cord and or its neuro‐vascular structures may increase and cause more leg pain and or hamstring tension.
Patients often present with slight forward (flexion) bending (the Phalen‐Dickson sign).
This posture leads to buttock pain as the gluteus maximus and medius and hamstring muscles become similarly engaged in protecting and stabilizing the lower back and hips through their myofascial attachments.
Clenched Buttocks
Over time this leads to a ‘chronic tight clenched buttocks’ often with spasms and pain.
This buttock clenching tension can often be seen clearly during examination.
Gluteal muscle spasm and tension can in turn lead to tension in the piriformis muscles, which engorge and then press upon the sciatic nerve (causing sciatica) or its blood supply (pseudo-sciatica).
Numbness is a common symptom and can be one sided or bilateral. It is usually felt down the back of the legs but this depends on where the spondylolisthesis is located.
Each nerve that exits the spine has a specific radiating pattern or dermatome.

Trigger Points
Often the leg pain is not directly related to pressure on the nerves but may be coming from muscular trigger points and associated tight muscles.
Tight muscles can press on the delicate blood supply to the nerves and mimic nerve pain (myogenic neuropathy). In these cases, trigger point therapy can be very, very effective.
Links
Find a Trigger Point Professional in your area
More Articles About Trigger Points
Dry Needling for Trigger Points
Certify as a Trigger Point Therapist

This trigger point therapy blog is intended to be used for information purposes only and is not intended to be used for medical diagnosis or treatment or to substitute for a medical diagnosis and/or treatment rendered or prescribed by a physician or competent healthcare professional. This information is designed as educational material, but should not be taken as a recommendation for treatment of any particular person or patient. Always consult your physician if you think you need treatment or if you feel unwell.
