
Rotator Cuff Injuries Explained

Pelvic, Trunk, and Scapula stability need to be secure to prevent common rotator cuff injuries
A survey of one year (2006) showed that over 7.5 million people visited their doctor for a shoulder problem, including shoulder and upper arm sprains and strains.
More than half of these visits (4.1 million) were for rotator cuff problems.
Rotator Cuff Explained - Jonathan Kuttner M.D.
Another more recent study (Lewis, 2014) reported that 70% of visits to doctors and therapists for shoulder pain were related to rotator cuff disorders.
Shoulder injuries are frequently caused by sports and athletic activities that involve excessive, repetitive, overhead motion, such as swimming, racket sports, throwing, and weight-lifting.
However, many of these injuries occur during everyday household and occupational activities such gardening, cleaning, and painting.

Anatomy
The group of muscles collectively known as the rotator cuff controls the motion of the head of humerus, the “ball” in the ball and socket joint of the shoulder (glenohumeral joint).
The “socket” part of the joint is the glenoid fossa of the scapula, so as the scapula moves so does the socket.
The rotator cuff muscles act to keep the ball of the shoulder joint secured in the right position in the socket.
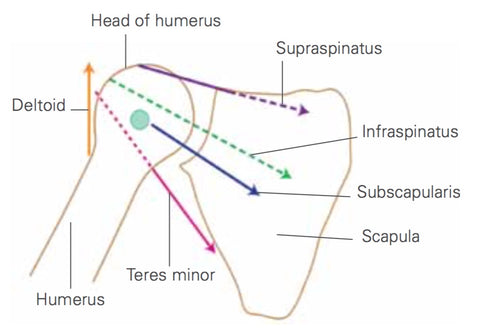
The rotator cuff group comprises supraspinatus, infraspinatus, teres minor and subscapularis. Each of these muscles has a unique primary action, but they also act together as a stabilizing unit.
When used for primary action, subscapularis acts as an internal rotator, infraspinatus and teres minor as external rotators, and supraspinatus as an arm abductor.
Movement and Stability
As stabilizers, these muscles exert a compressive force on the head of humerus to secure it in the socket during arm movements.
In effect they suck the head of the humerus into the socket, providing a stable axis for arm movement. Without the rotator cuff’s stabilizing action, the more superficial movement muscles pull the head of humerus across the socket as they contract.
The fixed point, or movement axis, is lost and the muscular pattern for force production and shoulder control altered.
If the head of humerus is allowed to slide up or forward in the socket, it can press against bony and ligamentous structures in the shoulder, causing tissue trauma and painful pathologies such as tendonitis and instability.
Correct and efficient rotation of the shoulder around its axis requires pelvis, trunk, and scapula stability.

Trigger Points
Trigger points, insofar as we accept them as part of the body's natural protect and defence mechanism, are often a good indicator of postural and stability issues.
Early identification and treatment is therefore always likely to be beneficial.
Trigger points make their host muscles shorter and weaker and trigger points in the rotator cuff muscles left untreated may lead to a number of painful shoulder disorders.
Injury Prevention
Rotator cuff training alone will not ensure shoulder health. Scapular stability is necessary to ensure that the socket is controlled and well positioned for whichever forces it must deal with.
Trunk and pelvic stability is necessary to provide a supportive foundation for the scapula. If your trunk stability is poor, it is likely that your scapulae will be dragged into a poor position.
Pelvic control problems can also alter scapular positioning, either directly due to excessive dependence upon latissimus dorsi, or indirectly by failing to provide a supportive platform for the trunk.
Treatment for Rotator Cuff Injuries
Symptoms of a rotator cuff injury include shoulder pain and loss of mobility. Often, these injuries occur in sports or as a result of an automobile accident. In other cases, they may develop due to the natural aging of the tendon. Regardless of the cause, a rotator cuff tear can lead to permanent loss of shoulder movement. However, there are many treatment options.
Depending on the severity of the injury, it can take several months to recover. Nonsurgical treatments can help relieve pain, but surgery is often necessary. Surgical procedures can involve arthroscopy (an incision that allows a surgeon to look inside the shoulder joint) or keyhole surgery. A doctor may also insert steroid injections to reduce inflammation. Both methods are effective in helping to relieve the pain and swelling associated with a rotator cuff injury.
Physical therapy may be recommended to strengthen the rotator cuff muscles and tendons. Some doctors may also massage the rotator cuff tendon to help relieve inflammation and pain. If the patient has a chronic injury, alternating heat and ice may be helpful. In addition, the use of cross-friction massage may be recommended. Physiotherapy can last up to six weeks. In the beginning stages, the therapist will show the patient stretches to do at home. The length of recovery will depend on the size and location of the injury.
Medical Investigation
X-rays, MRIs, and ultrasound scans are used to diagnose rotator cuff injuries. These imaging tests can be performed to check for bone spurs, inflammation, and other problems that can affect the rotator cuff. X-rays will also show if the humeral head is pushing into the rotator cuff space. If there is a degenerative change, rotator cuff surgery is an option. In some cases, a doctor can remove calcium deposits and bone spurs to treat the injury. Whether the rotator cuff injury is a result of a recent injury or a long-term degenerative condition, a doctor should be consulted as soon as possible.
In some cases, the rotator cuff is torn completely. In other cases, a small amount of the tendon may pull away from the bone. Large tears that occurred long ago are difficult to repair. The recovery time depends on the length of the tear, the age of the patient, and the level of activity. A rotator cuff tear can be treated with nonsurgical methods, but a larger tear may require surgery.
After the initial injury, the doctor will examine the patient's shoulder to determine the extent of the injury. He or she will also ask about activities that increase the pain. When the rotator cuff is torn, the patient may have trouble sleeping. Some people are awakened by pain during the night. If the patient cannot sleep, he or she should see a doctor immediately. In some cases, a doctor will recommend a sling to immobilize the shoulder. Slings can be removed at night.
After the initial injury, the doctor can refer the patient to a physiotherapist or other forms of appropriate natural therapy such as massage, acupuncture, trigger point therapy.
Summary
To protect the rotator cuff, make sure that your pelvic stability, trunk stability and scapular stability are secure in order to support good shoulder mechanics prior to performing resistance work for the upper body.
