
Manual Therapy - Understanding the Knee Joint
Talking about "Unexplained" Pain in the Back of the Knee
- Dr. Jonathan Kuttner M.D.
The knee joint negotiates the forces between the two longest levers of the body – the tibia and the femur. At first sight, it seems poorly designed and ill-equipped to cope with such varied and dynamic forces
The knee has been described as an "elbow designed by committee". The knee sits between the two longest levers of the body – the tibia and the femur – with most of the weight of the body coming down on it (and from various angles in a sporting context).
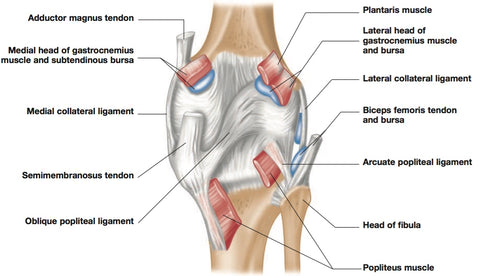
Right leg, Posterior View
At first sight the knee seems ill-designed to deal with such titanic and dynamic forces. For starters, the bones do not fit tightly with each other.
The femur ends in two rounded condyles, while the top of the tibia is described as a ‘plateau’; a fairly flat surface for the femur to land on.
This means that there is a certain amount of slide, glide and rotation available at the knee.
This makes for a necessary adjustability, but is not so great for stability.
Knee ligaments go a long way toward limiting the compromise.
The medial and lateral collateral ligaments allow minimal sideways (medial or lateral) sliding of the two bones on each other.
The lateral collateral ligament (LCL)
The LCL is under the iliotibial tract, running from the femur to the head of the fibula, which peeks out from under the tibial plateau.
This ligament is not part of the knee capsule, and is very strong and hard to break.
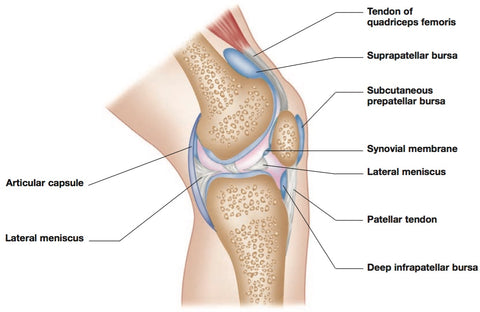
Mid-Sagittal View
The Medial Collateral Ligament (MCL)
The MCL is part of the knee capsule, making it therefore a bit arbitrary in terms of where we place the scalpel and say ... ‘This is part of the MCL and this bit right next to it is not.’
The MCL, though strong, is not as strong as the LCL, and is therefore more prone to injury.
This applies especially with young female athletes, where wider hip joints (on average) and athletic endeavor combine to direct more force into the medial knee.
Once weakened, the MCL can be a trouble spot for the rest of one’s life, so it is a frequent site for surgery.
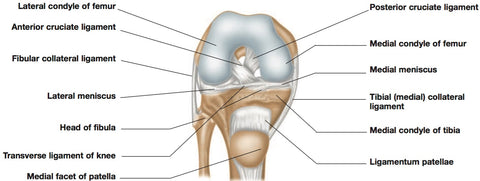
The other ‘crucial’ ligaments of the knee are the cruciate ligaments, so named because they cross in the center of the knee joint.
In spite of appearing to be in the middle of the joint, both cruciate ligaments, like the MCL, are simply stronger parts – thick and strong sections – of the complex knee capsule.
Anterior and Posterior Cruciate Ligaments (ACL and PCL)
The ACL and PCL prevent forward and backward sliding of the femur on the tibia, as well as locking in extension to prevent hyperextension of the knee.
There is nothing in the shape of the knee bones or patella that would prevent the knee from flexing to the front – this is the job of the ACL and PCL, which can be made too loose and overstretched by a sustained hyperextended standing posture.
The four major ligaments of the knee – medial collateral, lateral collateral, anterior cruciate and posterior cruciate – severely limit the side-to-side shearing of the two bones, and limit the front-to-back shearing enough to keep the two bones from sliding off each other in either direction. The cruciates also function to lock the knee from going into hyperextension.
Tearing or parting of the cruciate ligaments, especially the anterior one, is a not-infrequent football injury – it is, in fact, one injury that sent Moshe Feldenkrais on his quest for healing – and we all feel a little sick when we see a knee bent in the ‘wrong’ direction.
It is to the ligaments and not the bones that we must look for knee stabilization.
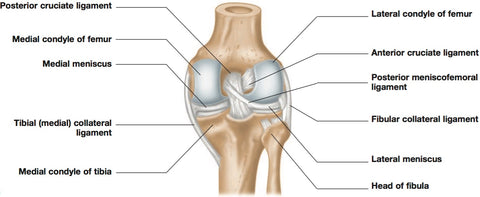
One last point about the ACL and PCL: they are arranged such that they loosen when the tibia is turned laterally on the femur, and tighten when the tibia is rotated medially, or when the femur is turned laterally on the fixed tibia.
Many of these knee-compromising injuries take place when the foot and lower leg are fixed on the ground and the upper body is turning into that knee.
Examples might include falling downhill over a ski, or that winning twisting backhand shot right after the foot is planted.
Cartilage
Both surfaces on the knee are well covered with thick cartilage, and there are additionally two menisci, semi-lunar cartilages that sit between the tibia and femur, and go a long way toward allowing the two surfaces of these bones to fit snugly with each other.
These cartilages lie loosely in the joint (though they manage to have connections with the cruciate ligaments and the medial hamstring tendons).
These C-shaped ‘rings’ of cartilage open when the knee is extended and the flatter end of the femur lies on the tibia, and close when the knee is flexed and the more rounded posterior part of the femoral condyles rest on the tibia.
This arrangement is great when it works, but for all the reasons cited above, these cartilages are subject to being frayed through grinding, or torn or cracked through shock injury.
They can even be folded over within the joint as a result of severe twisting.
Knee Joint Capsule
There is one more unique element of the knee joint that bears mentioning, because it shows what a marvelous piece of design the human body is.
The knee joint capsule, in addition to enclosing the area of the joint cartilages and menisci, has two extra ‘coves’ (see above).
One runs up in the front, under the patella, while the other sticks out the back of the joint and down, under the heads of the gastrocnemius.
The capsule cannot go out to either side because of the tight restricting collateral ligaments we described earlier.
When you put your leg forward, you contract the quadriceps.
This presses down on the patella, and the synovial fluid beneath it in the ‘cove’ at first cushions the patella, but is then squeezed through the joint into the back cove.
When you push off the foot a second later, you contract the gastrocnemius.
This is cushioned against the fluid, but then pushes that fluid back through the joint to the area under the patella.
In this way, the joint is lubricated very efficiently at both ends, and the large amount of cartilage in this joint is flushed and refreshed with its ‘food’, the synovial fluid.
Don't Run Before You Can Walk :)
Please note that this mechanism works best in walking, and not so well in running.
The best way to naturally care and feed a knee joint is to walk on it – if walking is not contraindicated – as this renews and repairs the cartilage.
Walking has about four million years of on-the-job training as a way of healing.
This is a solid and concrete example of how it works to renew us.
Links
Find a Trigger Point Professional in your area
Trigger Point Tools and Accessories
Dry Needling for Trigger Points
Certify as a Trigger Point Therapist
About NAT Courses
As a manual therapist or exercise professional, there is only one way to expand your business - education!
Learning more skills increases the services that you offer and provides more opportunity for specialization.
Every NAT course is designed to build on what you already know, to empower you to treat more clients and grow your practice, with a minimal investment in time and money.
Help Desk
About Niel Asher Education
Niel Asher Education is a leading provider of distance learning and continued education courses.
Established in the United Kingdom in 1999, we provide course and distance learning material for therapists and other healthcare professionals in over 40 countries.
Our courses are accredited by over 90 professional associations and national accreditation institutions including the National Academy of Sports Medicine (NASM) and National Certification Board for Therapeutic Massage and Bodywork (NCBTMB). Full details of all international course accreditations can be found on our website.
Printed course materials and other products offered on our websites are despatched worldwide from our 3 locations in the UK (London), USA (Pennsylvania) and Australia (Melbourne).
More About Us
NAMTPT AWARD 2017
We are honored to have received the 2017 "Excellence in Education" Award from the National Association of Myofascial Trigger Point Therapists.
Since 1999 Niel Asher Education has won numerous awards for education and in particular for education and services provided in the field of trigger point therapy.
Read Full Article
Award Winning Instructors
Niel Asher Healthcare course instructors have won a host of prestigious awards including 2 lifetime achievement honorees - Stuart Hinds, Lifetime Achievement Honoree, AAMT, 2015, and Dr. Jonathan Kuttner, MD, Lifetime Achievement Honoree, NAMTPT, 2014.
Meet the Instructors
NAT Certification
If you are a qualified/licensed manual therapist or exercise/fitness professional you can expand your credentials with NAT certification.
In addition to national accreditation for continued education, each course that we offer includes "NAT Learning Credits". By taking and completing courses you can accumulate NAT credits to qualify for NAT certification.
There are currently 3 levels of NAT certification. Certifying NAT is a valuable way to show your clients that you take continued education seriously, and to promote your skills and qualifications.
About NAT Certification
Accreditation
NAT courses are accredited for continuing education by over 30 professional associations in North America, United Kingdom, Australia, and European Union countries. These include The National Academy of Sports Medicine, Physical Therapy Board of California, AAFA, National Certification Board for Manual Therapists and Bodyworkers, Sports Therapy Institute, and Myotherapy Australia.
See Full List
Niel Asher Technique
Since 1999 the Niel Asher Technique for treating trigger points has been adopted by over 100,000 therapists worldwide, and has been applied to the treatment of a number of common musculoskeletal injuries.
The Niel Asher Technique for treating frozen shoulder was first introduced and published in 1997 and has been widely adopted by therapists and exercise professionals working within elite sports and athletics.
Read More
International Students
Most of our courses are available as either "Printed" or 'Download" editions. When you purchase a download edition, you receive immediate lifetime access to all course material. Course texts can be downloaded and printed if required.
When you purchase a "Printed" edition, you will also receive free access to the download edition.
We ship Worldwide from locations in the USA, UK, and Australia. Most items are despatched within 24 hours and shipping is FREE for all orders over US$50.
Shipping

This trigger point therapy blog is intended to be used for information purposes only and is not intended to be used for medical diagnosis or treatment or to substitute for a medical diagnosis and/or treatment rendered or prescribed by a physician or competent healthcare professional. This information is designed as educational material, but should not be taken as a recommendation for treatment of any particular person or patient. Always consult your physician if you think you need treatment or if you feel unwell.
